Who Ya Gonna Call?
June 20, 2023

It takes a village to raise a baby and support is key.
Breastfeeding can be extremely challenging and many people have never been around breastfeeding let alone babies.
New parents are often isolated not living near family and close friends. Because of this, the virtual world can be a welcome substitute, especially in the wee hours of the night.
When breastfeeding is not working the way you imagine it should it is easy to turn to your virtual village. The problem is that breastfeeding is a unique experience to each baby and their parent. There is no one size fits all way to feed your baby.
New parents are hungry for guidance. In their sleep deprived state they reach out: ”Help! My baby won’t latch.”
“Help! My nipples are bleeding,”
“Help! My milk supply is low,” and on and on.
Aunt Sadie scrolls through her feed and sees your SOS, “Just give that baby a bottle, don’t be a martyr.”
Your neighbor Steve says, “My wife downed the blue Gatorade and she spouted fountains of milk.”
Cousin Alex may offer, “Get a nipple shield, my friend who is thinking about becoming a lactation consultant told me that is works every time.”
These people are there in good spirit. They want to help but you are blasted with a barrage of anecdotes that may help some but do not address your specific situation.
You need a skilled professional to assess you and your baby, take a full history of your birth, your and your baby’s medical histories, and play detective to help you meet your breastfeeding goals. If you are struggling with breastfeeding reach out to an International Board Certified Lactation Consultant.

Fernando’s School of Latch Assessment
January 11, 2021
March 29, 2015
“It is better to look good than to feel good.”
Many mothers tell me that their breasts are painful and they want to know why.
“It could be the latch,” I offer.
“No, it is not the latch, the nurse/doctor/lactation consultant/my mother . . . (fill in the blank) said the latch looks great.”
The problem is that the mouth and tongue are complex and the movements are complex and can be effected by various outside factors.
Do you remember Billy Crystal as Fernando? His mantra was:
“Dahling, you look mahvelous! It is better to look good than to feel good and, Dahling, you look mahvelous!”

I believe that many health care professionals were trained to assess latch at Fernando’s Hideaway.
The latch is NOT marvelous if the mom is in pain. It is NOT marvelous if her nipples hurt, if the baby is not gaining weight, if the baby cannot maintain the latch for a feeding.
What can cause this poor latch?
There are a number of things that can make the latch un-marvelous. They can include:
- poor positioning
- birth trauma
- tongue-tie
- weak suck
What are the consequences of poor latch?
- breast infection
- low milk supply
- early weaning
- gassiness in baby
- fussy baby
- poor weight gain for baby
- engorgement
What can be done?
Understanding what makes a good latch. When there is a good latch both mom and baby comfortable and the baby moving milk appropriately.
Different remedies can help different challenges.
Positioning the baby close to mom is essential – the closer the baby the deeper the latch

If the baby is tongue-tied, this is where the frenulum that attaches the tongue to the floor of the mouth is too restricted, this small piece of skin can be released by surgical scissors or by laser.

This procedure is quick and can prevent a host of problems both immediately and down the road including poor weight gain, the need for orthodontia, digestive issues, premature weaning to name a few. Often when the tongue-tie is present there is also a thickened frenulum under the upper lip. This, too, should be evaluated.
If there is birth trauma healing can happen by bodywork by a practitioner skilled at working with babies.

This can include a chiropractor, a craniosacral therapist, an osteopath or a physical therapist. These folks are trained to help relieve muscle tension and to release the fascia. With birth trauma there can be misalignment in the babies oral structures. Sometimes the roof of the mouth is highly arched which can make the latch very uncomfortable as the breast tissue can be pressed into this area by the baby’s tongue. If this is the case often the baby feels tension and this makes his sucking more “chompy.”
Releasing the tension can help alleviate this pain and help to reorganize the baby.
If the baby has a weak suck there can also be therapies to help as well as suck training.
If there is a breast infection the mom can continue to nurse but she must be treated.

No matter what it is important to get the baby fed. It is also important to protect the milk supply.
When there is engorgement the mom can hand express, pump and/or nurse the baby.

When needing help with breastfeeding please do not accept that if it looks good then it is good. It should feel good and it should function appropriately.
If someone says “It looks good,” this is time to seek help by someone trained to assess the latch, inside and out.
In most cases that someone is an IBCLC – International Board Certified Lactation Consultant.
Working and Breastfeeding
October 13, 2018

I never met Kerry in person. We had one of those La Leche League Leader/Mom phone relationships. She initially called me with a few basic questions about breastfeeding her newborn. She then reached out to me as she was going to be working full time. She was having trouble pumping enough milk for her baby while she is away. I asked if it was possible to visit her baby during the day. We live in New York City and Kerry’s office was two subway stops away from her office – about a mile away.

Every Monday through Friday Kerry hopped on the train during her lunch break.
She had communicated with her nanny that she was on the way and that she would be nursing her baby.
This worked for Kerry and her baby as she had planned this in advance. Kerry communicated with her employer that she would take her lunch break out of the office. She communicated with her caregiver not to feed the baby a bottle at lunch.
Kerry was able to make up the difference with pumping while at work and at home in between nursing.
Employment outside the home is one of the biggest barriers to breastfeeding in the United States.
Does that mean it is impossible? No.
There are strategies and lifestyle decisions to consider.
What are the obstacles employed moms face?
- Maternity leave duration
- Time to pump
- Quality pumps
- Support from family and caregivers
- Support from employer
- Inconsistent information
- Balancing home and work life
Tina, an attorney, negotiated her maternity leave as well as her pumping schedule while she was pregnant and still working. She noticed that many of her colleagues returned to the grueling hours and were not breastfeeding when they returned to work. Tina laid out a plan for her firm and told them what she needed. This communication helped both her and her employer. They had never had a mom who was breastfeeding once she returned towork. Tina changed the culture of her firm. Some of those moms saw her as a champion and when they had a second baby they too had more success in breastfeeding.
Women are often told they need to sleep train their babies. That she needs to have her baby sleep in a separate room. If a baby sleeps for twelve hours and the mom is gone for nine hours that leaves three hours a day for them to be together. What is a mom to do?
Stacy, a physician, nursed her baby through her residency by keeping her baby in bed with her, despite criticism from her community. She was gone for twelve hours at a time. “How else would I get to know my baby?” she stated in delight.
Unfortunately, in the US standard maternity leave is twelve weeks. Sometimes moms will negotiate for more. Others will spread it out. For example, Lisa, a bookkeeper, returned to work at nine weeks for two days a week. It was early but it gave her an easier transition. She felt this allowed for her to slowly build up to five days a week instead of being home full time and then suddenly being gone all week.
Similarly, some moms who do need to return full time will have their first day back to work on a Thursday (if she works Monday through Friday) making this first “week” away a short one.
I am frequently contacted by moms of older babies of about three or four months of age. Breastfeeding was going well until two or three weeks back to work. Her milk supply is faltering and she cannot keep up.
She is pumping but the baby is flying through her stash.
Sometimes moms nurse and pump while on maternity leave and put themselves into an oversupply. They stockpile great volumes of milk and then when they head back to the office they rely on that stash. Even if they are pumping at work they may not be pumping as much as the baby is consuming. Then suddenly there is no more stash and the mom now has a low milk supply.

Some moms are truly not able to pump at work for various reasons so pumping during maternity leave is essential. For these moms it is important to nurse as much as possible when she and her baby are together. And she can add some pumping sessions in at home between nursing.
Many moms who are able to pump at work can enjoy the maternity leave without having to focus so much on pumping milk. As they transition back to work they can nurse the baby as much as possible when they are together.
To keep up and to reduce the need for more bottles and more pumping a mom can nurse her baby as the last thing she does before they part ways – either at the day care center or with the caregiver. She can then pump first thing when she gets to work to have one pumping session done. Then pump one or two more times during her workday. Then as she reunites with her baby the first thing she does is sit and nurse. This gives her and her baby the opportunity to reconnect and it also gives the opportunity for the mom and the caregiver to communicate. On days off the mom can focus on nursing her baby as much as possible.
Another challenge is the marketing of the faster bottles for older babies. This can undermine breastfeeding as the baby consumes more than he may need because the flow is faster. Once the baby has a bottle that works there is not need to move to a faster flow. Also, the caregiver can use paced bottle feeding to avoid overfeeding and flying through the milk.
Here are some strategies to keep nursing while working:
- Establish a good supply from the beginning
- Communicate with your employer
- Communicate with your caregiver
- Pump when you are away from baby
- Use a slow flow bottle
- Nurse your baby when you are with your baby
- Nurse all weekend (or on your days off)
- Pump as soon as you get to work (this gives you a jump start)
- If it is possible: visit your baby during the day so you can nurse
- Have your baby sleep with or near you
It is important to remember that breastfeeding is not just a way to get a baby fed. Breastfeeding is a complex relationship. By nursing a mother and her baby’s bodies are communicating. Bacteria are passed back and forth to build baby’s immune system. Hormones are passed back and forth to tell a mom’s body to make milk, to give her baby melatonin. There is feedback we do not entirely understand. And breastfeeding does not have to be all or nothing. If a person needs to supplement they can keep nursing for however much works for her and the baby. Working does not have to mean weaning.
Independence Day
July 4, 2018

Independent:
Not subject to another’s authority or jurisdiction, autonomous, free
Not relying on another or others for aid or support
Not influenced or controlled by others in matters of opinion, conduct, etc. thinking or acting for oneself.
On this, Independence Day, July 4th I cannot help but think of babies and their parents. There is such a cultural push to have babies become independent. There seems to be a fear of babies being too dependent on their parents. I hear the words “needy” “bad habits” “spoiled” bandied about in reference to babies’needs. But that is what they are: NEEDS.
Babies need to be held and fed and spoken to and socialized. They are not ready to be independent until at the earliest 18 years old.
Routine and structure are important but separation or rejection is not healthy. If you meet your baby’s dependency needs they will grow independent in time.




Nurse In
October 5, 2017
In 2005, Barbara Walters spoke on The View about her discomfort with nursing in public and particularly called out an incident on an airplane where a woman nursed her baby next to Ms. Walters. A group of parents and activists gathered outside the studio in a peaceful protest. I was pregnant with my third baby and was excited to be part of this nurse-in. http://www.nytimes.com/2005/06/07/nyregion/lactivists-taking-their-cause-and-their-babies-to-the-streets.html
Much has changed over the last decade. Breastfeeding is promoted by celebrities and is seen as a good thing generally speaking.


As an IBCLC I mentor up and coming Lactation Consultants.

I was contacted by, Perrine, one of my interns last week. She told me that her friend was asked to move and to cover up at a store in Columbus Circle. Perrine is from France and wanted to know what the rules and laws are in the US and NYC.
The laws are clear, you have a right to breastfeed where you have a right to be in NYC.https://www.nysbreastfeeding.org/laws-and-legislation/
My first thought was, “we need a good old fashioned Nurse In!”
Perrine was thrilled. Thrilled to be able to stand up for her friend, to do something that could effect change and to take action.
It was easy to put together. A quick Facebook event and a bit of sharing.
Last Friday, September 29, just before 10:00am I arrived at the Shops at Columbus Circle and the first thing I noticed just outside the store were these beautiful twelve foot Adam & Eve sculptures by Botero.
They are impressive bronze statues that are nude. Of course, Adam & Eve are nude.
I find it ironic that a woman wanting to feed her child in the most normal manner is told to turn away so no one can see her while twenty feet away from these colossal nudes.


By 10:10 several moms and babies arrived at the atrium and gathered in the shadow of the Botero sculptures. A camera man from a local news station walked into the mall. I asked him if he was there for the nurse in. He was but told me he could not film inside the mall. We walked outside the mall and he began to focus his camera on me. A security guard approached us and told the camera man he could not film there. The camera man told him he had cleared it with head of security and to go ask him. As the guard swiftly went in search of his boss I spoke into the camera. I told whomever would be listening that it is important to normalize breastfeeding and that people should not be shamed for feeding their babies. I said that the breast is overly sexualized and that people in our culture cannot separate the sexual from the simply functional.
Back inside as we all gathered I was approached by a man in a suit whom I assume was the head of security for The Shops. Our exchange went something like this:
Him: Hi, what is going on here?”
Me: “Oh, my friends and I are going to do some shopping at Williams Sonoma. And, we may feed our babies if they get hungry.”
Him: “alright.” He nodded his head and smirked a knowing smirk.
We walked into the festively decorated shop, it smelled of cranberries and roasted turkey. We were offered tastes of their mulled cider. It was delicious.
A baby started to wiggle and her mom said her baby was ready to nurse. We were standing next to a beautifully appointed table and I asked an employee if my friend could sit and feed her baby. She smiled and replied, “of course.”
Then other moms pulled out the chairs and nursed their babies. It was beautiful and peaceful and ordinary. I watched the moms one by one get comfortable in their act of “defiance.” A bit sheepish at first then, one by one, easing into a setting of just a few moms sitting around talking and nursing and admiring the beautiful décor.
I asked if I could take their pictures. One of the moms was at first shy about being photographed and then as time went on she said, yeah, I can be photographed. She smiled and looked up at me and said, “I am a Lactavist!” She held her head a bit higher and she beamed at her baby and at herself.



I decided to “out” us. I asked the woman who allowed us to use the table and chairs if I could speak to a manager about an incident that had occurred earlier in the week. She seemed genuinely disturbed that there was an incident and got the manager immediately.
August is a tall man with dark hair pulled into a neat ponytail. He approached me and when I told him of the Perrine’s friend he was upset. He wanted to know which employee it was who had made this mom so uncomfortable. He assured me that the store policy is that a person can feed their baby anywhere and they do not have to hide or cover up. This was heartening and I wondered if I had made a big deal out of an isolated incident.
I approached the moms some of whom were nursing their babies and others whose babies had drifted off into milk drunkenness.
When I told them they were happy. They commented that they were happy to be a part of something.
I realized this is important for them, for the store manager, for the employees, the head of security and the channel 7 camera man.
This was not a big rally but it had an impact. The ripple effects will carry on. The social media sharing that happened continued throughout the week. Every little bit makes a difference. I cannot be quiet when it comes to social justice. I may not always have the right things to do or say but I will not sit idly by and let people be harassed for feeding their babies.
We quietly dispersed, I went home, got my gear and went to see a couple of families in their homes to help them feed their babies. Just another Friday!
To Pump or Not To Pump
July 26, 2017
This is a question many new parents are faced with. People do not realize the amount of information thrown at new and expecting parents until they are expecting and new parents themselves.
One of the big decisions parents have to make is how they are going to feed their baby. It seems like most Americans consider breastfeeding. There are many obstacles that interfere with breastfeeding – that is a post for another day but let’s talk pumping milk.
I recall when I was pregnant with my first baby I took a breastfeeding class. I knew I wanted to breastfeed but did not have many role models so I listened intently on how to breastfeed. I remember the instructor talked about pumping and how it is best to rent a pump – I am not sure I remember much more. When Phoebe was born I struggled with how to get her latched and how often to feed her and I had a striped scab across one of my nipples and a hickey on the other from her latching onto the areola. I remember in a fit of frustration telling Rob WE NEED TO RENT A PUMP! NOW!
It took a few days for us to figure out how and where to rent a pump – this was 1995! Phoebe and I found our rhythm – she found my nipple I found how to listen to her cues. The pump arrived and I stared at it.

For three and a half weeks. We rented it for four weeks. I knew I needed to use it before returning it and having spent over $80 renting and buying parts. I put the shields on my breasts and was impressed that milk came out of my breasts.
Later that night Rob came home from work. This was summer and there had been a storm. The electricity was out. Phoebe started to root around. “You have to give her this bottle! Now! My milk is going to go bad and we do not have a refrigerator and it is 99 degrees!”
Rob grabbed the bottle and tried to feed our screaming baby. I walked out of the room. My breasts began to tingle and leak. Rob was sweating, Phoebe screamed louder and louder. Her head spinning like Linda Blair in the Exorcist. I started to cry. I think Rob was crying, too.
“Give me the baby.” I latched her on and we both chilled out.
“What do I do with this?’ asked Rob.
“Pour it down the drain,” I told him.
It turns out I did not need to pump. The company I was working for went out of business so I became a full time mom.
I asked Rob if he felt he needed to feed Phoebe to bond. He laughed and told me he felt bonded with here.

And eventually I became a La Leche League Leader and then a Lactation Consultant (IBCLC).
As someone who has been in the breastfeeding business for two decades I have seen different trends. With the Affordable Care Act offering up pumps to expecting parents and with social media there is a big pumping culture. And there is so much information shared that it can all be confusing.
If your baby latches on, you feel comfortable and your baby is gaining weight there is no need to pump.
Conversely, I have seen women who were told not to pump for two weeks or for one month or whatever someone told them was a rule. Or no one told them to pump while their baby is being supplemented with formula. In some of these cases this compromises their milk supply. The bottom line is that the baby must be fed. But if your baby is being supplemented and you want your body to make milk then it is important to pump. Milk is made by removing milk form the breasts – this can be with a baby who has a good latch, by hand expressing or by using a good breast pump.
Let’s now talk pumps. Pumps are not all created equally and not everyone responds to pumps the same. I have worked with people who pump using their hands – hand expressing – here is a cool video:

There are hospital grade pumps, electric single user pumps , and hand pumps.
When should you pump?
- If your baby is separated from you
- If your baby is not gaining enough weight
- If your baby causing you so much pain you cannot tolerate nursing
- If your baby takes a bottle
- If you are donating milk
- If you are working away from your baby
There is no need to fill your freezer! Pumping is not an Olympic sport!
How many people compare their milk stash to those they see on Instagram?!
You really only need enough milk to feed your baby.
If you want to pump that is cool but if you do not want to pump and do not need to then don’t pump.
People can bond with a baby without a bottle. If you want your baby to have a bottle of breastmilk, then pump.
Each situation is unique and blanket statements do not help new parents. For help call an IBCLC (International Board Certified Lactation Consultant) Find a Lactation Consultant or a La Leche League Leader.La Leche League International
Lactation Education Nirvana
June 9, 2017
This week I was in lactation nirvana.
On Tuesday I attended an all day conference on TOTs – this is Tethered Oral Tissues – this includes tongue tie, lip tie and buccal tie. The conference was put together by Dr. Scott Siegel, a physician and dentist who is uses laser to release these ties. The event was multidisciplinary with sessions given by and attended by IBCLCs (International Board certified Lactation Consultants), SLPs (Speech Language Pathologist) CNMs,(Certified Nurse Midwife) OTs (Occupational Therapist) Orofacial Myologists, doulas, and more.
I have been in Private Practice as an IBCLC for 15 years. I have worked with hundreds of tongue-tied babies and even nursed two tongue-tied babies. I learned so much and more importantly had explanation for the things I knew instinctively and saw in my practice but could not quite explain. I have a better understanding of the impact of TOTs on people of all ages.
Wednesday night I attended a reading of the book, The Big Letdown by Kimberly Seals Allers. The subtitle is How Medicine, Big Business and Feminism Undermine Breastfeeding. I live this book everyday. The obstacles against breastfeeding are immense. They keep coming. As we solve one issue another pops up.
I was asked by a journalist yesterday to answer a few breastfeeding questions. One was “Does my ethnicity affect my ability to breastfeed?” My gut response was, “heck, no! Mammals are mammals.” But the reality is that breastfeeding is a learned and cultural experience.
What needs to happen is that families need to be supported on many levels. Education is imperative. There are so many obstacles. (More on these later.)
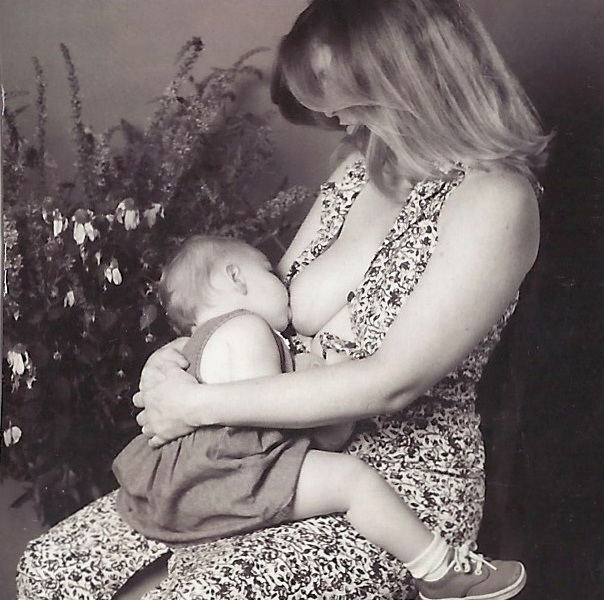
Sometimes I get weary of the repetition of some of the problems that could be resolved with education and normalizing breastfeeding. I never get weary of empowering and educating families. And I NEVER get weary of holding babies.
I will continue to help families, educate myself and keep sharing my knowledge – even when met with resistance.
Tandem Nursing
August 10, 2016

Tandem Nursing means nursing two babies at once. This can be twins or it can be siblings born at different times i.e. an toddler and an newborn.
Many people believe that you cannot get pregnant while nursing or that if you are nursing when you are pregnant you need to wean.
You can get pregnant while nursing.
Breastfeeding can be birth control under specific conditions. There is the Lactational Amenorrhea Method (LAM).
LAM works like this:
- No return of menses since birth
- breastfeeding on demand, night, and day
- baby does not take any food or other liquids regularly
- baby’s sucking needs met primarily at the breast (no pacifier or bottles) baby is less than 6 months old.
- baby does not go longer than four hours during the day and longer than six hours during the night between nursing
With LAM there is about a 1-2% chance of getting pregnant – similar to taking birth control pills.

Many people get pregnant while nursing. Often moms are advised to wean their older baby if they become pregnant. There is no need to wean unless you are at risk for premature labor and you are advised by your health care provider to refrain from intercourse.
What can you expect while nursing while pregnant?
About halfway through pregnancy your milk changes from mature milk to colostrum. Colostrum is thicker and does not flow as easily as mature milk. Some toddlers get frustrated and wean. Others hold on for dear life!
One telltale sign of pregnancy can be sore nipples. Some moms find nursing painful or they become averse to nursing and they choose to wean their older baby.
Others will put limitations on nursing – one mom used counting as her strategy – “you can nurse for ten seconds – 10, 9, 8 . . .“ Another mom had a nursing chair where they could only nurse sitting in the chair in a quiet room.
Some advantages of tandem nursing can be:
- nursing toddler can help relieve engorgement
- older baby not feeling left out
- mom doesn’t feel she is abandoning the older child
- she still has her magic toddler wand
- sibling bonding
- stronger immune system of the toddler
Disadvantages:
- mom may feel touched out
- judgement from family, friends and health care team
When nursing twins it can be a good idea to alternate breasts for the twins. This can be every feeding or everyday – Twin A gets the left breast while Twin B gets the right breast for one feeding and then alternate the next feeding or on Monday Twin A gets left breast and Twin B gets right breast and on Tuesday Twin A gets right breast and Twin B gets left breast and so on. Many moms of twins will choose to nurse one at a time once they get older to have one on one time. In the early days it can be a time saver to nurse both at once.

How does one manage tandem nursing babies of different ages?

Weaning
June 23, 2016
I remember when all three of my children weaned.
My plan for Phoebe was to nurse for one year.
I figured I could avoid formula and bottles if I nursed her for twelve months.
At my baby shower for her I received 36 bottles! I had not registered for anything and told people I would be breastfeeding. We did not have a dishwasher. The thought of washing bottles overwhelmed me and made me want to breastfeed even more.
Laziness was a motivating factor initially in some of my parenting choices. Breastfeeding and co-sleeping were the bomb!
Though we struggled together initially, nursing became an extension of my mothering Phoebe.
As her first birthday approached I got anxious about the weaning process. How would I do it? Who would it benefit? How would I calm a tantrum or get her to sleep?
The Last First Day
September 9, 2015
This morning as I dropped off my youngest child at school I was weepy. Was this Kindergarten or PreK? No, this was fifth grade. Finn is over five feet tall. He has been going to the same school since her was four years old. Why was I weepy? This marks the end of an era for me – as a mom, as a community member, as someone who is seeing time go by in my middle years.
This is my last First Day of School at the Earth School.

My first First day of Earth School was in September of 2000. For the last fifteen years I have been trekking up and down Avenue B in the East Village of New York City

Just north of 14th Street is Stuyvesant Town where we live. I have walked in snow, sleet, rain and in the blazing sun to get to our beloved elementary school. I have walked with babies in my belly, babies in slings and babies in strollers. I have seen teachers come and go and some come back! I have been through three principles. I have fund raised and recruited other families. I have escorted countless field trips often with a toddler in tow!

At Earth I have found community. I have met some of my closest friends. My family has forged relationships with other families with whom we share holidays and birthdays.
I remember the first annual Earth School Auction.
I have enjoyed the art on the walls and read some inspiring poetry and memoirs by the wonderful children who populate the halls and hearts of our community.
I remember when the roof garden was an idea and then it became real.
I have seen families grow and I have seen families leave. I have seen tragedy and great joy and simply ordinary days at Earth. I was at Earth that terrifying morning on September 11, 2001.
I have watched children perform on the stage.
I have nursed babies in the halls and in the lobby. I have sold popcorn and cookies in the lobby. I have done on-the-spot lactation consulting in the lobby.
I have grown as a human at Earth. I have watched my children grow and thrive. I have seen them learn to tie their shoes and learn conflict resolution and learn to construct a sentence and to defend an original idea.
I have learned about community building and about celebrating the seasons by marching in Tompkins Square Park to celebrate solstices and equinoxes.

I learned about what education is. I have learned so much more. I have learned to let go and watch my babies grow into smart, confident people.
In nine months my youngest child will graduate from the Earth School. But today is the first day of fifth grade for Finn. I will embrace this day and open my heart to the Earth community.
